Achilles Strain / Rapture
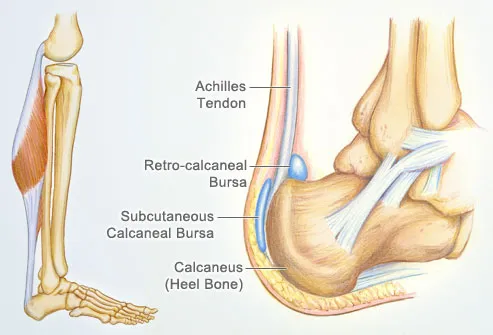
The Achilles tendon is a strong non-elastic fibrous tissue that connects the calf muscles to the calcaneus (heel bone). It is also the largest tendon found in the human body and helps an individual to engage in everyday exercises like walking, jogging or running. Notably, when calf muscles contract, the Achilles tendon tightens, hence pulling the heel, for a movement like walking to take place (Pedowitz & Kirwan 2013). The tendon is further located at the back of a leg, where it runs from the heel to the calf as seen in figure 1 below. The tendon attaches the gastrocnemius muscle and the soleus muscle to the calcaneus. An Achilles strain or rapture hence occurs when the tendon completely tears or otherwise raptures.
Read also Parents Should Not Let Their Kids Play Football Due To The Serious Injury Risks?
The Achilles tendon is significantly strong and can withstand ground reactive forces of up to 6-8 times the body weight, at an average of 800 foot strikes/mile. A tear or rapture of the tendon is often a result of overuse or, age, inadequate footwear, abnormalities resulting from conditions like gait among others. Nonetheless, there are other extrinsic factors like use of drugs with corticosteroids and fluoroquinolones, which are known to weaken the Achilles tendons, thus increasing the risk for a strain when conducting basic physical activities like walking, running or jumping (Sode et al., 2007).
The severity of this particular injury is defined by the nature of the rapture or tear. In many instances, people tend to experience a slight tear, which is an incomplete tear that may go unnoticed until the individual cools down from an activity. Partial tears are more prominent than complete rapture of the Achilles tendon and is often misdiagnosed as a sprain (Pedowitz & Kirwan 2013). Notably, raptures to the Achilles tendon are very common in athletes who constantly load the tendon while preparing to push off. This can happen when there is a sudden change in direction when the athlete begins to run or jump, and is a result of a tremendous force generated by the calf muscles through the Achilles tendon to propel the body forward. Another way to injure the Achilles tendon would be through acute force trauma, where an individual’s Achilles tendon is literally cut off by a sharp object either accidentally or during a violent encounter. Nonetheless, this method is very rare.
Other common mechanisms of injury include a sudden forced plantar flexion, a violent dorsiflexion of a plantar flexed foot, as well as a sudden dorsiflexion of the foot. A forced plantar flexion is very common and can occur when a person stretches out to pick an item from a high shelf, in ballet dancing when dancers use the tip of their feet and even when people wear high heeled shoes (Pedowitz & Kirwan 2013). On the other hand, dorsiflexion of the foot is experienced when walking or even pressing on a car peddle. In rare cases, some patients get Achilles tendon rapture from attrition of the tendon due to preexisting peritenonitis regardless of a tendinosis present.
Anatomy of the Injury
An Achilles tendon structure is made up of an extracellular matrix and thin, cylindrical cells. These cells include tenocytes and tenoblasts, which are responsible for synthesizing components of the extracellular matrix (Paavola, 2001). The matrix consists of elastin and Type-I collagen which gives the tendon strength. Additionally, the collagen contains ground substance which consists of glycosaminoglycans and proteologycans (Ahmed et al., 1998). The tendon is surrounded by an elastic sleeve called the partenon, which works to allow free movement between the surrounding tissues. Further, the partenon is made up of cell layers which transport blood in the tendon.Given that there exists very few blood vessels, the blood flow in the tendon is poor hence elongating the period of recovery following a trauma (Carr & Norris 1989). When the Achilles tendon raptures, a patient feels the pain and may experience inability to push off when starting to run, jump, walk or tiptoe. The rapture often splits the tendon into two, a factor that requires immediate medical attention.

Signs and Symptoms
When a person raptures the Achilles tendon, they would first experience a sharp pain at the point of rapture and throughout the ankle. A person is also likely to hear a snapping sound. All other preceding symptoms will be felt within the immediate surroundings of the tendon. Notably, pain is often felt above the heel, when an individual stretches the ankle or tries to stand on toes (Pedowitz & Kirwan 2013). The area of rapture may also feel swollen, stiff and tender. Alongside the pain, patients with the injury report experiencing bruising and difficulty pointing the toes as well as pushing the toes forward to walk. Those who manage to walk, do so with a marked limp. In the case where the rapture is partial, the pain may be mild but will get worse if neglected. Additionally, upon rapture, the sharp pain experienced may subside quickly, hence risking a misdiagnosis where doctors may be led to diagnose a sprain. Other symptoms of the injury include morning pain, which occurs as a result of stretching as well as exacerbation of the injured location when walking uphill (Pedowitz & Kirwan 2013).
Diagnostic Procedures
A diagnosis of the injury always begins with a subjective assessment to determine the mechanism of the injury. In this case, a physician provides a report of pain in a location of about 2-6 centimeters proximity to the Achilles tendon to determine the affected areas of the foot. This method is effective but often times leads to misdiagnosis as a strain, especially when the raptured area is swollen and difficult to feel the inside of the tendon (Pedowitz & Kirwan 2013).
A more objective approach involves a full examination of the lower limb. By assessing the knee and the hip, doctors get clues on the biochemical aspects that result from muscle imbalances. Further, an examination of the foot involves observation for swelling, joint effusions, asymmetry and atrophy (Pedowitz & Kirwan 2013). Physicians also check for palpation in the form of tenderness, and localized pain in the affected regions to identify the exact location of injury, anatomic deformities as well as areas where the patient experiences pain.
A diagnosis of an Achilles tendon rapture is often reached if the physician feels a disconnection of the tendon after feeling the calf muscles and surrounding areas of the Achilles tendon location (Pedowitz & Kirwan 2013). In the case where a physical examination is unclear, doctors use ultrasound or an MRI scan to examine the interior of the Achilles tendon location as a means to identify any deformities, rapture or strain.
Basic Healing Process
The healing process is based on the patient’s approach to treatment. While some patients prefer non-operative treatment methods, others confine with surgical treatment options. Both methods have pros and con, a factor that leads to the diversity in the treatment selection amongst patients. Physicians advise patients to highly evaluate their overall health goals, their activity levels and rehabilitation expectations before selecting one of the two approaches.
The most common non-surgical treatment involves the placement of a cast from the knee to the toes, in a way that the foot points upwards (Chutkan, 2013). The cast is later replaced with shorter casts over a period of time, in a process that often lasts 6-12 weeks. The doctor will also regularly move the foot until it is back to normal. On the other hand, the surgical approach often follows the percutaneous or open technique. Using the percutaneous technique, the surgeon creates small skin incisions to repair the raptured tendon (Chutkan, 2013). With the open technique, the doctor makes an incision on the injured part to better the view and proximity of the tendon. The healing process after the surgical approach also involves the placement of a cast or postoperative boot to help the patient move.
Regardless, the treatment option, patients are expected to protect the injured area to ensure effective healing, regularly move the ankle and foot to stop loss of muscle tone and stiffness, and minimize load by observing their recommended physiotherapy exercise.
Rehabilitation
Patients who opt for non-surgical treatment methods risk experiencing a re-rapture, given that prior studies show the rate of re-rapture in these patients is three times higher than patients who opt for surgical treatment (Chutkan, 2013). Nonetheless, non-surgical treatment options have also shown early motion protocols as compared to surgical treatment which is characterized by delayed motion protocols which may result from wound complications in patients. Both the surgical and non-surgical methods have similar rehabilitation strategies. After the casting period, patients using both treatment approaches are expected to begin physical therapy. Patients who opted for the conservative approach often begin earlier than patients using the surgical approach. The physical therapy is initiated to restore motion and reduce stiffness.
The rehabilitation protocol for athletes is more specified and aligned with normality objectives wherein the athlete may regain the ability to play or run effectively within a short period of time. To this regard, most athletes select a non-surgical approach as their first choice for treatment. After surgery, the rehab protocol often involves personalized care wherein a nurse is assigned to dress, remove stitches, and adjust boot lock to a specified flexion degree and control pain and edema within a given period of time (Chutkan, 2013). The injured athletes are further engaged in physiotherapy exercises which begin with mild activities like straight leg raises, and gradually increase to increased weight bearing exercises over a twelve week period.
Conclusion
In sum, the Achilles tendon is the strongest tendon in the human body. A rapture or tear of the tendon often occurs over time as a result of overuse. Additionally, many other extrinsic and intrinsic factors play a role in the development of events leading to injury. An Achilles tendon rapture is painful and may restrict movement of the leg and heel, hence requires immediate treatment that would allow for healing. There are two forms of treatment, surgical and non-surgical. Both treatment approaches have pros and cons. Nonetheless, the healing process using both procedures takes about 6 to 12 weeks (Chutkan, 2013). Patients are also expected to rest the injured leg, engage in physiotherapy and exercises as advised by the doctor. While the Achilles tendon is very strong, a strain or rapture is not uncommon especially to athletes.
Order Unique Answer Now
Organisms in the Domains Bacteria and Archaea
The Role of Intelligence Sharing in Global Counterterrorism Strategy